|
Don't leave Fido at home  For those having a hard time with their health, feeling lonely or in want of an unbiased listening ear, an animal can be a balm to the soul. So how can the smallest and softest on this planet make an impact on the oldest and toughest among us? And how can animals be included in the day to day lives of those in Aged Care and Independent Living and Retirement Villages across NZ? Who can resist petting a soft, fluffy animal? I’d wager that the soulful eyes of a cute pooch could soften the heart to even the crankiest human. In fact, studies show that just 15 minutes with a dog, cat, or other animal can increase brain activity and serotonin levels in seniors. Being able to bring a pet with you can be a make or break for people choosing to leave their own home in the community and relocate to a village. For those who are widowed, their pet is more than just an animal. It’s their sole form of day-to-day company. For people who aren’t so interested in being socially engaged, it can be even better than a human. Are all villages on board with bringing pets along? One of the reasons John (name changed) settled on his Retirement Village was that he could bring his feline friend Mittens (name changed) along, when he moved in with his wife from their large family home to a more sensibly sized independent living townhouse. Mittens had more or less chosen to move in with John some years before, after abandoning her owners for the affection and food on offer at his house. Although feisty at times, John and Mittens became good buddies, especially appreciated when his wife was away. Not keen to leave his home, John agreed to move eventually as long as Mittens was in tow. Ryman Healthcare allows residents who live independently to have pets, so when someone is moving in and wants to bring a pet, they meet the manager to ensure they are appropriate, and then get written into the contract. John’s townhouse has a convenient cat flap, and his neighbours also keep cats. In fact their shared love of feline company encouraged fresh friendships with those around him as they chatted about their animals.  So in what capacity can animals be found in villages? There are recent heart-warming stories of cats adopting villages. As we all know, cats have staff, not owners so it makes sense that they like to choose their own abode. During the covid lockdown of 2020, Coco the cat chose to move into Rita Angus Retirement Village in Wellington. Cruising the hallways during the day, Coco enjoys plenty of attention from the residents and she’s totally charmed the security guards. Bella is the Maygrove Hospital cat. By day she’ll snooze in the office, by night she roams the hospital. Night staff make sure she is fed, but she still tries her luck with getting extra from the day staff – especially a creamy treat! Another cat who’s cottoned on to the benefits of retirement village living is Digby who arrived at Wairarapa Village in Masterton with his owner. Eventually his owner passed away and Digby was adopted by the village, who now keeps an HR file on Digby. The feline resident does daily rounds of the occupants and happily rests in their gardens. If a facility won’t allow your traditional cat or dog (or fish or parrot) – are there other options? One of the most unusual surfaced back in 2014. The NZ Herald reported on Auckland’s Selwyn Heights retirement village who had purchased four robot seals known as “Paro” for residents to interact with. A trial carried out at the facility found residents were less lonely and more engaged after sessions with Paro. Could robots have a future in healthcare? Robotic animal love could bring a faux version of physiological benefits similar to the real things but without the ongoing inconvenience of buying food or taking them outdoors for a walk on a rainy day. There may be an untapped target group for the likes of FurReal Friends Pets Toys -if they can stimulate the brain of a growing kid, then why can’t a robotic seal help lower blood pressure and improve Grandad’s day?  If you live in a village where they have a non-replacement pet policy and your fur-child passes on, what other options are there for bringing a fluff-bomb of love to your doorstep? Maygrove Village in Orewa allows residents to have a pet as long as it is not a nuisance to others, fully vaccinated and leashed in common areas, but they have also had a positive experience with therapy animals. The hospital on site has pet therapy visits as well as a resident cat who lives there. Toni Hatton, Assistant Manager at Maygrove says “The pet visits are incredible. We even have a horse called Peanut who visits sometimes. She’s great in the lift, well toilet trained but does not like to get back in her float to leave, she would rather graze on our lush lawns! The hospital/palliative residents just adore her” – Peanut isn’t the only horse being kept busy with animals. Tyson the therapy horse visits the elderly and terminal patients in the Tasman district and provides a quiet connection to people when no words are needed. Originally Tyson would stand outside but graduated indoors to visit those too sick to venture out of their rooms. An organisation who offers beneficial animal encounters is Canine Friends Pet Therapy. They specialise in pet therapy by facilitating canine visits at hundreds of retirement homes, hospitals, hospices, universities and even businesses across New Zealand. As the name implies, they specialise in therapy dogs and aren’t picky about size or breed, but the dogs do need to pass an assessment before being accepted into the programme  It's a basic concept, patting a pet = good for us! But overseas in England they’ve taken it one step further with a more innovative approach than just a few pats to a furry face, and it’s something that could easily be taken up here in Aotearoa, particularly now that eggs are at a premium. ‘HenPower’ brings together older people and hen-keeping to combat loneliness and depression and improve wellbeing. Found in more than 40 care homes, HenPower creatively ‘hengages’ older people in arts activities and hen-keeping to promote health, wellbeing and reduce loneliness.
So, if you’re looking to move into a Retirement Village and want to bring Rover don’t assume it’s a no-go. Check your top choice is a pet welcoming facility, and, importantly, what their replacement policy is for pets. If Rover dies, can you have another Rover Jnr? If not, talk to your activities manager about pet therapy visits, or if that fails maybe you’ll be in luck and they’ll buy some robotic pups (or real life hens) to pat. Ref: Aged Advisor NZ NZ’s Best Magazine Under pressure: The science behind weighted blankets and stress relief The idea is simple: the pressure of the blanket simulates the feeling of receiving a hug. From Aged Care New Zealand Issue 02 2022  Simple yet effective, the weighted blanket is an impressive innovation in relieving anxiety and symptoms of other conditions. The idea behind it is simple: the pressure of the blanket simulates the feeling of receiving a hug. For many weighted blanket users, this leads to relief and calmness. But this innovation is far from new. In the 1980s, Temple Grandin, a scientist and animal behaviourist, discovered the benefits of pressure sensation. To make the beef industry more humane, Grandin observed that frightened cows would regain calm after being pushed tightly into a squeeze chute, for example. From these observations, she went on to develop a hug machine that duplicated this calming pressure. This was the first developed to ease the symptoms of autism, a diagnosis that Temple Grandin shares. Recently, there has been a resurgence of interest in this sensory therapy modality, with weighted blankets becoming popular in the mainstream. Let’s look at everything you need to know about weighted blankets – and if you could benefit from using one. What is a weighted blanket? A weighted blanket is a therapeutic tool similar to a conventional blanket in all but its weight. Often, they weigh anywhere from 2kg to 13kg. The blanket is often filled with glass beads or plastic pallets. The concept? The blanket is heavy enough to exert pressure on you much like getting a long-lasting hug after a rough day. Who can use a weighted blanket? The short answer? Anyone can use a weighted blanket. Regarding more specific use cases, occupational therapists who work with kids tend to use weighted blankets as a treatment option for sensory activities. This can include various conditions such as autism or attention deficit hyperactive disorder (ADHD). This easy-to-use tool may also help with the following:
Recent research efforts have focused on better understanding the mechanism of weighted blanket therapy for relieving the symptoms of the conditions mentioned above. In 2020, Swedish researchers conducted a study to determine facets of that effectiveness. They found that weighted blankets improved sleep among people with ADHD, generalised anxiety disorder, bipolar disorder, and depressive disorder. So how do they work? The mechanism of how weighted blankets work is not well studied or understood currently. Weighted blankets are used in therapy as part of the sensory integration therapy model. This model is based on integrating inputs from two systems:
The main benefits of using a weighted blanket provide security and comfort Swaddling a newborn baby helps them sleep soundly at night, and this is because of the sense of security the tight swaddle provides. A weighted blanket works under a similar principle, helping you sleep securely and comfortably throughout the night. Reduce stress and anxiety levels Stress and anxiety are the most significant contributors to interrupted sleep. Constant worry and fear make it hard to fall asleep during the night. In turn, sleep deprivation can aggravate an individual’s anxiety levels – so it’s essentially a vicious cycle. A weighted blanket helps by applying pressure to soothe your anxiety and help you rest.  Improve sleep quality Some research studies have demonstrated the benefit of weighted blankets on improving sleep and reducing the impact of insomnia. The mechanism behind this is not yet known. However, it is thought to be mediated by serotonin, cortisol, and melatonin hormones. The pressure created by the blanket’s weight can go a long way toward improving your overall sleep quality. Calm the nervous system Weighted blankets help restore calm in your nervous system by applying even pressure on your body. Sleeping with an overactive nervous system can be challenging. Luckily, weighted blankets are a quick and effective means of overcoming this hurdle. According to a study, 63 per cent of participants stated that heavy blankets helped lower their anxiety levels after just five minutes of use. How to choose the best weighted blanket for you. As the COVID-19 pandemic continues, stress and anxiety are still taking centre stage, causing many of us to revisit our mental health. That said, a weighted blanket might be a great tool for you. So, how do you pick the best option? Consider the following factors. Blanket weight The average weight of weighted blankets ranges from 2kg to 13kg. You should select a weighted blanket that weighs no more than 10 percent of your body weight. Weighted blankets for children weigh close to 2kg, and adult blankets range from 2kg to 13kg. Consider getting a lighter blanket for users with mobility issues. Although the pressure of the blanket has its benefits, it can be unsafe to apply too much pressure with a weighted blanket that is too heavy. That’s why the 10 per cent rule is recommended. If you have any concerns or questions about which weight is right for you, speak with your doctor or ask to be referred to a therapist who specialises in sensory integration therapy.
Weighted blanket material Weighted blankets are filled with two types of material: plastic pellets or glass beads. Glass beads are smaller – but heavier than plastic pallets. That small size has an advantage in that the blanket appears thinner. In contrast, plastic pellets are bigger, making the blanket a bit bulkier. However, blankets with plastic pallets are considerably cheaper since plastic is inexpensive compared to glass. Some weighted blankets come with other materials, such as polyester fibrefill or fleece lining, for an extra layer of warmth. If you’re planning to use the blanket during the cold winter months, this might be a nice perk. Removable cover Due to the weight of the blankets, they are bulky and hard to wash, which means a removeable cover is ideal. Cotton covers make for cool, breathable blankets, while other fabrics may best suit that warm and cosy feel. Sometimes, sellers will price covers as an add-on, so never assume your blanket comes with a removable cover. Adapted from an article by Esteban Vaquera. Medically reviewed by Brittany Stopa, MPH. Available at: www.symptomfind.com Top Tips for a Tidy Transition Leaving a family home can be as much an emotional disconnection as a physical one. But at what point does the cost of emotional connection to a house outweigh an older adult’s wellbeing?  Suzi Brown explains Leaving a family home can be as much an emotional disconnection as a physical one. The family home might be where you brought your brand-new babies home to, where they were raised, where celebrations and commiserations were experienced. But at what point does the cost of emotional connection to a house outweigh an older adult’s wellbeing? It’s inevitable that at some point it will become more clear that the season for your family to enjoy the security of that home has passed. Time to pass the property baton to other whanau to flourish under its roof. The question is, HOW does one even begin the process emotionally or physically, without being buried under a mountain of unneeded but previously loved possessions? Let’s investigate. Robyn from Transition Navigators, an organisation who works with elders to find the accommodation that best fits their needs, stresses the importance of not underestimating the time it takes to talk through the options to arrive at the right choice. Ideally, it should be a conversation started in your late 50’s or early 60’s. She comments that everyone’s Plan A is always the best scenario, which is rarely the reality. Plan B involves the reality of planning and saving for a successful outcome. Think of it this way, we spend lots of time transitioning children from one important step to the other - preschool – primary school – higher options, but where is that transition planning and support at the other end? Do your sums The best strategy is to start by asking the difficult questions and doing some basic maths for comparison. While staying in your own home may mean you're saving on some things; also remember that moving into a retirement village means you can budget all the expected fees ahead of time; and you don’t need to worry about rates. For example, as part of ‘Ryman’s Peace of Mind Guarantee’ for independent living and serviced-apartment living, your basic weekly fee will never increase, unless you change your living arrangements or add extra aged-care options. Their fixed weekly fee for independent living covers maintenance, services and lifestyle (social time and happy hour, their activities programme). You can enjoy the benefits of disposing of those annoying tasks like washing windows and organising building insurance. If you need someone to change your light bulb, simply call up the maintenance man and it will be done. For some people, removing that to-do list equals independence more than remaining in their own community home. Let the professionals help If figuring this all out is just a bit too overwhelming, there are businesses who specialise in helping through this process. The beauty of using an outsider is that they aren’t emotionally involved in your life, so they have the benefit of viewing your situation from a fresh angle. They can assist with de-cluttering and navigating your move. I sat down for a quick chat with two experienced women who provide practical solutions through their businesses which specialise in this area. Transition Navigators With a warm and welcoming twinkle Robyn is experienced in helping older people and their families make informed choices. Her organisation works with older people who are planning to downsize from their family home, or with families when a health crisis signals a change in circumstance. Her role is to research the best options and work with older adults and their family to navigate a smooth transition. Robyn has a wealth of useful experience, with a PhD on the wellbeing of independently living older people – both those living in retirement villages and in the community. Neat Spaces Helen’s business, as a Professional Organiser, works alongside elders, helping bring more order and efficiency while de-cluttering and managing life transitions. Her services include setting up sustainable systems, storage solutions, creating usable spaces, paper management and deceased estate assistance. Your own private Marie Kondo with a reliable touch! What about all that dreaded ‘sorting out’? If moving house looks like the best solution. It could be time to tackle a monstrous sort out session. Downsizing from a family home full of memories is an emotional time, so how do we identify what to keep, and recognise what to donate or sell? How do we navigate the emotional upheaval of letting go of items steeped in memories? Once again, this is something that takes time. Ideally we need to start this task early, thinking about what items are really important to us and then communicating that with our children or loved ones. Maybe you need to ask what sparks joy for them and be able to give them these items in advance. Belongings that were really important to previous generations can hang a heavy mantle of responsibility on your shoulders. If you don’t want these items, and neither do your children then some difficult choices need to be made. Although you might feel a bit silly, you could try the Marie Kondo approach of holding the item, thanking it for its use and value for a moment, and then releasing it. If you’re going through this process with your elderly parent, remember to show empathy and listen to the associated stories, even if you’ve heard them plenty before! Helen from Neat Spaces likens the process to an onion – peeling one layer at a time. She notes there is a fear around the connection of letting possessions go, meaning letting memories go. Often clients think when they donate or sell an item, they’re letting go of all the special memories, but in taking time to say goodbye you can retain those memories. Find peace from moving into a new season. A new space can provide the fresh appeal of a less cluttered environment which will result in a less chaotic mind.  Anyone heard of ‘Swedish Death Cleaning’? Once again the Swedish have found a fabulous way to do something boring much better than anyone else on the planet. Heck, they probably look gloriously tanned, blonde and beautiful doing it too. The idea is this: once you reach the end of middle age (or round about that time), you quite simply just get rid of stuff that’s built up and not needed anymore so that no one else has to do it once you pop your Crocs. In Sweden, it is called döstädning – dö meaning “death” and städning meaning “cleaning.” The 2018 book by author Margareta Manusson called “The Gentle Art of Swedish Death Cleaning: How to Free Yourself and Your Family from a Lifetime of Clutter” centres on this topic and is touted as “a charming, practical, and unsentimental approach to putting a home in order while reflecting on the tiny joys that make up a long life.” Apparently Manusson’s method makes the process uplifting rather than overwhelming, so it could be worth a look if you’re in the market for inspiration. Her book reminds us that once we’ve decluttered, we’ll be able to focus better on the really important things in life. Once the decluttering is complete, you’ll feel less stressed as a reflection of less mess on the outside. The reality of the whole process of Swedish Death Cleaning is that getting rid of items reminds us that things don’t last forever, including us, and wouldn’t you rather be the one to make the choices about what happens to all your stuff, than some other person who might just biff it all in the skip? Stay put Check out all your options. Could you stay put for another few years with the addition of services coming into your home? To know if you should stay or go officially, your GP team or a community health worker can refer you for a needs assessment. These exist to find out whether you need support, and to assess the most suitable support you specifically need. The support services could cover:  Personal care such as getting out of bed, showering, dressing and helping you with your medications
A good place to start for services are Access Community Health, Healthcare New Zealand or Nurse Maude (Christchurch only). What place do we choose? In the industry they’re known as “The Big Six” – Ryman, Metlife, Summerset, Bupa, Oceania, and Arvida. They are significant players in the New Zealand Retirement Village market, and between them they have an estimated 43% of villages throughout the country. You might have a natural inclination of which one you’d like to investigate due to location, amenities or already having friends in that particular village, but if you’re a bit unsure which direction to turn we have a handy suggestion! www.agedadvisor.nz is an independent review website specialising in aged care. The benefit of visiting Aged Advisor is that the reviews are completely unbiased by the companies themselves. Search up your top choices and read reviews from people who actually live in the villages or aged care facilities without the skew of village marketing. There are also helpful articles and due to the success of their retirement village reviews, the website will be expanding into funeral, legal and financial reviews. Don’t forget to pay it forward when you’re all settled in your lovely new abode by writing your own review on your chosen provider too. Remember to be empathetic to yourself when making your final choices, but also remember to weigh your choice up with the concern it would cause your loved ones. At the very least, maybe get a bit of Swedish Death Cleaning underway, and reduce the trip hazards in your home whilst also preparing to relocate. Give your choices time, talk the options over and you’ll be sorted, tidy and in no time. Ref: Aged Advisor NZ NZ’s Best Magazine Financial Planning for Retirement Those clever planning types (you know the ones, they’re good at spreadsheets) set the example by getting ahead of the game. But for those amongst us who are more of the creative, ‘fly by the seat of your pants type’, how do we arrange finances so we don’t arrive at 65, 75, 85 then wonder how to afford a few tea bags and a reasonable haircut? Suzi Brown explains Each decade or season of life brings an opportunity to get your financial ducks in an organised row, so you can continue enjoying the kind of lifestyle you’ve enjoyed during working years, in your retirement.  To begin the process, it would be helpful to have a dollar figure goal in mind. But considering we’re not given a definite number of years at birth, how on earth can do we work out how much we’ll need? Stats NZ Tatauranga Aotearoa’s latest report shows life expectancy at birth has continued to increase. They now project males to live to 86.1 years and females to 89 years by 2050. In researching this article, I stumbled upon a somewhat grim-reeperish, yet necessary tool which has been created called the ‘How long will I live calculator’ on the stats.govt website. Basically, you enter the year you were born, your age and sex and kazam! There’s your answer, divided helpfully into three categories assuming low, medium and high death rates. You’ll also need to decide whether you’d like to live a no frills or extravagant retirement lifestyle or sit somewhere in the middle with enough popped aside for the odd splurge if the opportunity arises. It’s really an essential first step for smart retirement planning – overestimate your longevity on the one hand and you could leave retirement too late or live too frugally, but underestimate and you could be low on funds. The table overleaf, put together by Massey University, gives you an estimate of the type of figure you may need to work toward. This amount depends on the number of people in your household, whether you’ll be aiming for a no-frills or ‘choices’ type of retirement and your location. Once you’ve figured out your sobering estimate of years left on earth and broken down how much you might need, it’s time to write some lists. Start with jotting down the things that are important for you to do now, and that you’d like to continue doing when you stop paid work. Then – this is the fun bit – add the things you have always wanted to do during retirement. Don’t be afraid to be extravagant at first! That’s what a budget is for. Write down that fancy cruise you’ve always dreamed of. It might mean you have to scrimp and save, or maybe buy second hand a bit more, but keep your end goal in mind and do what you need to do to get to those big ticket items – YOLO (you only live once)!  Where do your dollars and cents actually go? It’s smart to be organised when spending, to allow for as much saving opportunity as possible. Think about: Renewing subscriptions: sift through your credit card statements carefully and check for subscriptions you don’t need or didn’t even realise you were still paying for. Planning meals and grocery shopping – regular meals out or last-minute takeaways can really impact your pocket. Plan your weekly meals and shop accordingly to save those hangry dashes at the drive through! Prioritise paying off high-interest debt – be wary of purchases that offer monthly payments with interest. Does your spending match your goals and values? – keep your core values at the forefront. Before you pull out your EFTPOS card ask yourself if the purchase you’re about to make lines up with what’s really important to you. 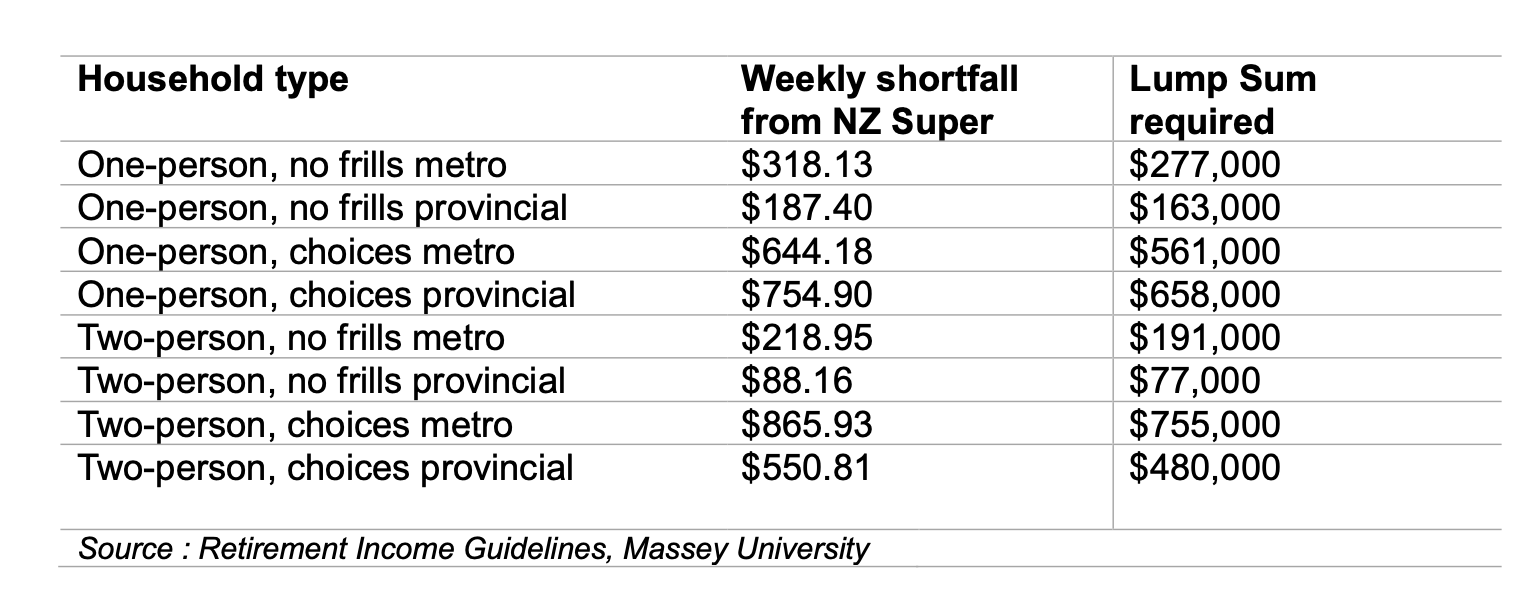 Why not earn a few extra bucks? Around a third of Kiwis continue some form of paid work past age 65. It’s a great way to add a few more dollars to cover your daily expenses, as well as keep some social connection and continue to feel a sense of value. Think about finding an opportunity which allows more flexible hours, part time or casual work, consultancy or mentoring, and the great thing is, income from paid work will not affect your entitlement to NZ Super. Your house is an asset It’s a really good idea to think ahead about where you're planning to live once you’ve hit the golden age of retirement. If you’ve been living in your family home for some time, selling with the intention of purchasing a cheaper one can free up some money while still providing the benefits of owning a home. If you plan on downsizing and moving to a rural area, keep in mind there are trade-offs – consider your social network and access to health services before committing. Some other ideas to make some money off your home are:
Preparation by decade How old are you now? How much time do you have left to prioritise the big save? You could make this easier for yourself by breaking it into the financial priorities for each decade of life. If you’re mid child-rearing then it’s not prime time for really pulling your socks up, but if you’re heading toward 60 then you’ll need to get amongst it. 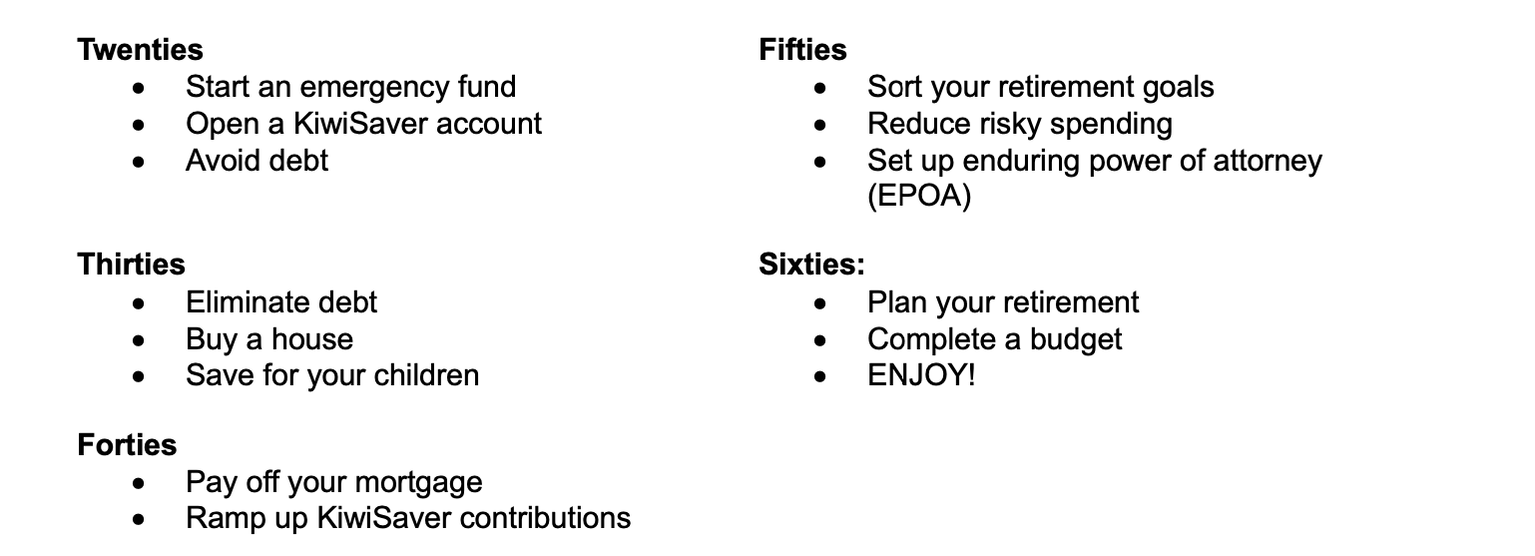  Tools to help you prepare
Sorted.org.nz website – you’ll find all sorts of tips and tools to help you handle your money well! Get a financial adviser – they can help you define your goals and objectives, take into account your personal circumstances; and develop a plan; you can start by looking for one at financialadvice.nz/find-an-adviser Chat to your KiwiSaver provider – they may offer financial advice or provide you with a financial adviser who can help you work out what is the right fund for you. Ref: Aged Advisor NZ NZ’s Best Magazine Music Therapy Week  Music Therapy New Zealand (MThNZ) is delighted to announce the upcoming Music Therapy Week, aligning with the World Federation of Music Therapy’s (WFMT) Music Therapy Week, from 10th – 15th April 2024. The 2024 theme ‘Looking Back Moving Forward’ serves as a poignant reflection on the rich history within the music therapy profession, honouring the dedicated individuals and co-collaborators working towards the growth of music therapy in New Zealand. For Music Therapy Week 2024, MThNZ is excited to offer the opportunity to interview registered Music Therapists from across Aotearoa. These passionate professionals will share their insights into why music therapy is crucial for individuals and communities. MThNZ’s purpose is to champion potential and well-being through the professional use of music therapy. As a therapeutic practice, music therapy is carefully planned to assist the health and personal growth of individuals with identified needs. Registered music therapists possess highly honed skills to work with a diverse range of conditions, including physical and intellectual disabilities, neurological conditions, mental health and mood disorders, and substance abuse issues. The adaptability and versatility of music therapy enable its application in various contexts such as schools, community spaces, hospitals, care and supported living facilities, prisons, and private practices. Sarah Cole, Executive Officer of Music Therapy NZ, emphasizes, “In Aotearoa, music therapy is increasingly being used to assist in general wellbeing, providing support for those living through the challenges of trauma, separation, grief, and end-of-life care.“ The WFMT’s initiative for a World Music Therapy Week (WMTW), celebrated annually from the 10th to the 15th of April, highlights the global connectedness of music therapy. This event encourages music therapists and supporters worldwide to engage in activities that raise awareness and advocate for the therapeutic benefits of music. Sarah Cole notes, “Music therapy transcends borders, and the global recognition through World Music Therapy Week emphasizes the collective commitment to improving lives through the power of music.“ “New Zealand contributes significantly to the worldwide trend of success for clients through music therapy. Our passionate and highly skilled therapists are dedicated to utilising music to enhance the lives of individuals facing diverse challenges. As a country, we strive to be at the forefront of promoting the global connectedness and therapeutic impact of music therapy.“ Liz Wallace Music Therapist at Therapy Professionals has recently published an article on her work with people with an Intellectual Disability which may assist your understanding of how music therapy works in practice. Read Liz's article here
Also take a look at Radio New Zealand's recent segment on music therapy and how it is helping to build confidence in children. https://www.rnz.co.nz/national/programmes/ninetonoon/audio/2018933828/using-music-therapy-to-build-confidence-in-children Connecting with your community to enhance wellbeing Acute isolation has the same effect as hunger on the body from Aged Care New Zealand Issue 1 2022  As the pandemic has swept through countries around the world, life as we know it has been shaken up in unprecedented ways. Constraints on our daily activities to keep ourselves and each other safe has come with not only an economic but also a social cost, as people deal with lockdown fatigue, anxiety around falling sick, and more. Social isolation and loneliness have been widespread issues for a long time, but it has become much more pronounced across a range of groups since the COVID pandemic arrived over two years ago. In fact, pre-pandemic surveys show that one in five pensioners in NZ living at home felt extreme loneliness. As bleak as these statistics are, the social isolation and restrictions on movement have also presented opportunities to take a more conscious approach to how we manage our wellbeing. About social isolation and loneliness Although the terms are often used interchangeably, there are two separate definitions for social isolation and loneliness. Social isolation describes the amount or quantity of social interaction one has while loneliness describes the quality of one’s social interactions. In essence, this means that it is possible to feel lonely even with regular social interaction and on the flipside, people who do not require and don’t have high levels of social interaction don’t always experience loneliness. However, it is common for social isolation to be a precursor to loneliness. Social isolation and loneliness have been shown to be detrimental to both physical and mental health. During the pandemic, loss of face-to-face interaction, including family time, religious services and social clubs has been felt acutely, particularly by older populations. In addition to the emotional pain of loneliness, research is exploring the impact on physical health as well. Some of the adverse effects linked to loneliness include increased risk of diseases and disorders such as dementia, heart disease, stroke, cancer and functional decline. One study showed that acute isolation has the same effect as hunger on the body. Because loneliness can cause stress, elevated levels of the stress hormone cortisol has been observed in people who experience prolonged loneliness. This in turn causes inflammation in the body and leads to increased risk to physical health. These harmful effects of social isolation and loneliness are the rationale for taking action to improve our wellbeing. Fortunately, there are a few easy ways to change things up and reach a happier, more fulfilling mental state. Looking after wellbeing during a pandemic During the pandemic, many places turned to technology to connect with loved ones from afar. Religious services and healthcare have also gone digital, and many older people adapted well to these changes. Even if newer technologies such as video calling may not be everyone’s forte, phone calls are still a great alternative. Lockdowns and social distancing have compelled us to be creative about the ways we connect with each other and to take stock of the ways we keep ourselves happy and healthy. A more holistic way of taking care of our wellbeing comes from the Māori health model Te Whare Tapa Whā, devised by Sir Mason Durie. This model uses a whare (house) to describe four pillars of wellbeing: taha wairua/spiritual wellbeing, taha hinengaro/mental and emotional wellbeing, taha tinana/physical wellbeing and taha whānau/family wellbeing and social wellbeing. Our connection with the whenua/land forms the foundation. When the pillars and foundation of the house are strong, so is our wellbeing. 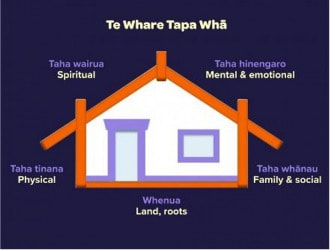 Some ideas for tending to each pillar:
While it may seem daunting initially to incorporate new changes into our lives, it can also be an exciting opportunity to extend ourselves and see what benefits can occur from stepping out of our comfort zone. How others are connecting since COVID Over the last two years the Mental Health Foundation and All Right? have been working on developing the Getting Through Together campaign to spread wellbeing messages during the pandemic. As part of the campaign several people shared their stories of how they were connecting with each other from afar. Sharing the love At level three of lockdown Steven would drive to the rest home, where his wife resided. He parked up below her window and displayed hand painted signs. “It wasn’t easy, but the hardest thing was rattling around at home all by myself and knowing she was less than five minutes drive down the road.” John and Jill At 83 and 81 respectively, John and Jill say the COVID 19 crisis was unlike anything they have experienced. The modern conveniences of 2020 meant that the pair managed to create online versions of their normal day to day life. Their 10 grandchildren and three step grandchildren all kept in touch via FaceTime, “at a higher rate than they might normally have heard from them,” Jill grins. Jill also has wine group that’s been meeting every second Friday for the past 30 years, and there was no way COVID 19 was slowing that down, with the group reconvening over Zoom every fortnight instead. John’s weekly walks with his group of friends, followed by a long lunch turned into frequent phone calls and email chains, and he even found a solution to missing his trips to the Christchurch art gallery – overseas galleries like The Metropolitan Museum of Art in New York offered virtual tours around their exhibitions.  More support
While we always recommend that you speak to your family doctor or GP for any health-related concerns, if you’re looking for more resources, support, and further information, here are some useful places to start. To chat with a trained counsellor 24/7, free call or text 1737. The Mental Health Foundation of New Zealand works towards creating a society free from discrimination, where all people enjoy positive mental health and wellbeing. Resources and information are available from the web shop at shop.mentalhealth.org.nz or call 09 623 4812. Age Concern New Zealand is a charity providing expert information and support services in response to older people’s needs. There are many local branches throughout the country to service local communities. To get in touch, you can visit the website www.ageconcern.org.nz or freephone the national office at 0800 652 105. Yellow Brick Road (formerly Supporting Families) is a charity that provides mental health support for families who have a loved one experiencing mental health challenges. They are experienced in supporting carers. Visit their website at yellowbrickroad.org.nz. Let’s End Loneliness is a project to tackle loneliness and create communities in which New Zealanders have the relationships they need to thrive. Their website letsendloneliness.co.nz features resources and create communities in which New Zealanders have the relationships they need to thrive. Their website letsendloneliness.co.nz features resources and initiatives to foster social connection. Mental Health Foundation Ref: Aged care Issue 1 2022. Recruiting high quality aged care workers The recruitment process can be long and overwhelming, but don’t let that get in the way of finding the right person. From Aged Care New Zealand Issue 02 2022  Aged care workers play a critical role in the care experienced for older citizens, so finding the right employee is imperative. The following are some tips on how to attract the ideal candidate and what to look for in a potential employee. Attracting applicants The backbone of a successful aged care facility with a high standard of care is having high quality, passionate staff. The challenge many facilities are facing is where to find such candidates. One way to optimize the potential to find the right fit for your facility is to align yourself with a training provider. There are three main recruitment approaches that could result in excellent outcomes through this partnership:
Once you have implemented one or perhaps all these processes with the goal to find suitable candidates for long term employment, it is important to remember what it is that will make an exceptional member to your staff. Quality and skills Regardless of the method used to find an applicant, it is useful to know what quality and skills you are looking for to make the right recruitment choices. Soft skills are highly regarded in the aged care sector and any new job applicant should be able to demonstrate that they possess these skills. Examples of soft skills include patience, compassion, empathy, communication, emotional intelligence and problem-solving. There are various soft skills that make an applicant more suitable to an aged carer’s role, so selecting and outlining which are of the highest value for your facility could help save time in the recruitment process.  Soft skills are often characteristic of those who are particularly interested in caring for others. The possession of these skills is part of what makes an exceptional aged care worker and will in turn improve the overall level of care that your facility provides.
While formal education is important when considering prospective employees, some educational gaps are not necessarily problematic when on the job training can be provided. In fact, an advantage for an applicant who has had extensive formal training is to also have had practical hands-on experience where theory was applied to real life situations. Aligning values Each aged care facility will have its unique values and it’s important to find employees who can align themselves with the values of your facility. Often people are attracted to caring for others for altruistic reasons, so outlining the morals and values that your facility holds in high regard may assist in finding the right candidate. Employment in a rewarding role and in an environment that reflects your morals and values will contribute to staff wanting to remain in the position long term. Elderly residents and staff in aged care are often from culturally and linguistically diverse backgrounds. To provide the highest most comprehensive care for an increasingly diverse population, it’s crucial to consider the applicant’s ability to ensure every individual is treated with dignity and respect, and their identity, culture and diversity is valued. Members of staff with practical capacities, compassion and understanding will support your facility to become more culturally competent and it will consequently meet the needs of the residents and staff more holistically. Dispelling myths The range of misconceptions about working in aged care propagated by the media are well-known myths that have led to negative views of the industry and have contributed to shortage of aged care workers. These inaccurate descriptions ignore the positive influence aged care workers have on the lives of elderly people who are unable to live on their own. Staff in aged care communities often find it an extremely rewarding career, one that is not limited to personal care of the elderly but includes undertaking advanced care and treatment such as rehabilitation, mental health support, and activity management. Addressing these more realistic points in an interview and communicating the important and positive aspects of working in aged care can alleviate an applicant’s concerns, especially for those just entering the field. This is a good opportunity to highlight the supportive culture that your facility fosters for the health and wellbeing of the staff. Finding the right person to join your aged care team may be time consuming, but taking the right steps is important. By aligning your facility with a training provider to attract job seekers and having a clear idea of what you will look for in a candidate are important parts of the process. Following these ideas may save you both time and money in attracting and hiring the right person for the job. Blueberries and strawberries slow cognitive decline People who eat greater amounts of blueberries and strawberries could delay their cognitive aging by years according to data from a large-scale study conducted over more than three decades. From Aged Care New Zealand Issue 02 2022  In a paper published in the journal Annals of Neurology, German and US researchers report that cognitive decline could be delayed by up to two and a half years in elderly people who eat more of the flavonoid-rich berries. Flavonoids are compounds found in fruits, nuts and vegetables that have been linked to disease prevention through their antioxidant and anti-inflammatory properties. Berries are particularly high in a type of flavonoid called anthocyanidins, which can cross the blood-brain barrier to areas of learning and memory. The research team used data from the Nurses’ Health Study, which has collected information about the diet of 121,700 female, registered nurses since 1980. Between 1995 and 2001, the team measured cognitive function in 16,010 women over the age of 70, at two-year intervals. Those who ate more berries experienced a delayed cognitive decline by up to two and a half years. But the authors stressed that while they did control for health factors in the modelling, they could not exclude the possibility that participants with preserved cognition may also have been affected by lifestyle choices, such as exercise. Study leader Elizabeth Devore, from Brigham and Women’s Hospital and Harvard Medical School in Boston, said that because the US population was ageing, understanding the health issues facing the elderly was vital. “Our findings have significant public health implications as increasing berry intake is a fairly simple dietary modification to test cognition protection in older adults,” Dr Devore said. Bryce Vissel, Head of Neurodegeneration Research Laboratory at the Garvan Institute of Medical Research in Sydney, said the public policy implications of the research were “sufficiently important to merit further study. However, the implications are further reaching, as they show that research offers the possibility to identify ways to slow dementia. Most importantly, if research can show that lifestyle affects cognitive decline, then it seems logical to suggest that research will also deliver effective treatments that slow cognitive decline, given the chance.” Dr Vissel added: “The potential implications of this type of research are that simple berries could potentially reduce the time before elderly people may need care. However, the broader point is that more research is needed, and it is needed urgently.” Flavonoids appeared not only to influence cognitive function but also visual function, said Peter Howe, a Research Professor in Nutritional Physiology at the University of South Australia.  “What I think is happening here, which is not considered in this paper, is that the flavonoids are acting on the blood vessels in the brain and the eyes to improve the circulation. We’re conducting research at the Nutritional Physiology Research Centre looking at how foods rich in flavonoids, like the ones present in these berries, are able to improve blood flow in the brain, because that may be the key to their cognitive benefits.”
Shawn Somerset, an Associate Professor of Public Health at the Australian Catholic University in Brisbane, said that in elderly Australians the most likely source of flavonoids was wine. Berries were expensive, he said and there were other good sources of anthocyanidins, such as aubergine. “Australians intake of vegetables is inferior to fruit, therefore vegetable consumption needs to be promoted above fruit consumption.” “The most sensible advice is to consume a wide range of flavonoids, rather than large amounts of specific ones, since excessive amounts of some are problematic. This translates to consuming a range of vegetables and fruits, not just one type.” Author: Justin Norrie This article is republished from The Conversation under a Creative Commons licence. Read the original article here: theconversation.com/blueberries-and-strawberries-slow-cognitive-decline-6684 Reference: Aged Care NZ Issue 02 2022 Under pressure: The science behind weighted blankets and stress relief The idea is simple: the pressure of the blanket simulates the feeling of receiving a hug. From Aged Care New Zealand Issue 02 2022  Simple yet effective, the weighted blanket is an impressive innovation in relieving anxiety and symptoms of other conditions. The idea behind it is simple: the pressure of the blanket simulates the feeling of receiving a hug. For many weighted blanket users, this leads to relief and calmness. But this innovation is far from new. In the 1980s, Temple Grandin, a scientist and animal behaviourist, discovered the benefits of pressure sensation. To make the beef industry more humane, Grandin observed that frightened cows would regain calm after being pushed tightly into a squeeze chute, for example. From these observations, she went on to develop a hug machine that duplicated this calming pressure. This was the first developed to ease the symptoms of autism, a diagnosis that Temple Grandin shares. Recently, there has been a resurgence of interest in this sensory therapy modality, with weighted blankets becoming popular in the mainstream. Let’s look at everything you need to know about weighted blankets – and if you could benefit from using one. What is a weighted blanket? A weighted blanket is a therapeutic tool similar to a conventional blanket in all but its weight. Often, they weigh anywhere from 2kg to 13kg. The blanket is often filled with glass beads or plastic pallets. The concept? The blanket is heavy enough to exert pressure on you much like getting a long-lasting hug after a rough day.  Who can use a weighted blanket? The short answer? Anyone can use a weighted blanket. Regarding more specific use cases, occupational therapists who work with kids tend to use weighted blankets as a treatment option for sensory activities. This can include various conditions such as autism or attention deficit hyperactive disorder (ADHD). This easy-to-use tool may also help with the following:
How do weighted blankets work? Recent research efforts have focused on better understanding the mechanism of weighted blanket therapy for relieving the symptoms of the conditions mentioned above. In 2020, Swedish researchers conducted a study to determine facets of that effectiveness. They found that weighted blankets improved sleep among people with ADHD, generalised anxiety disorder, bipolar disorder, and depressive disorder. So how do they work? The mechanism of how weighted blankets work is not well studied or understood currently. Weighted blankets are used in therapy as part of the sensory integration therapy model. This model is based on integrating inputs from two systems:
The main benefits of using a weighted blanket provide security and comfort Swaddling a newborn baby helps them sleep soundly at night, and this is because of the sense of security the tight swaddle provides. A weighted blanket works under a similar principle, helping you sleep securely and comfortably throughout the night. Reduce stress and anxiety levels Stress and anxiety are the most significant contributors to interrupted sleep. Constant worry and fear make it hard to fall asleep during the night. In turn, sleep deprivation can aggravate an individual’s anxiety levels – so it’s essentially a vicious cycle. A weighted blanket helps by applying pressure to soothe your anxiety and help you rest. Improve sleep quality Some research studies have demonstrated the benefit of weighted blankets on improving sleep and reducing the impact of insomnia. The mechanism behind this is not yet known. However, it is thought to be mediated by serotonin, cortisol, and melatonin hormones. The pressure created by the blanket’s weight can go a long way toward improving your overall sleep quality. Calm the nervous system Weighted blankets help restore calm in your nervous system by applying even pressure on your body. Sleeping with an overactive nervous system can be challenging. Luckily, weighted blankets are a quick and effective means of overcoming this hurdle. According to a study, 63 per cent of participants stated that heavy blankets helped lower their anxiety levels after just five minutes of use. How to choose the best weighted blanket for you. As the COVID-19 pandemic continues, stress and anxiety are still taking centre stage, causing many of us to revisit our mental health. That said, a weighted blanket might be a great tool for you. So, how do you pick the best option? Consider the following factors. Blanket weight The average weight of weighted blankets ranges from 2kg to 13kg. You should select a weighted blanket that weighs no more than 10 percent of your body weight. Weighted blankets for children weigh close to 2kg, and adult blankets range from 2kg to 13kg. Consider getting a lighter blanket for users with mobility issues. Although the pressure of the blanket has its benefits, it can be unsafe to apply too much pressure with a weighted blanket that is too heavy. That’s why the 10 per cent rule is recommended. If you have any concerns or questions about which weight is right for you, speak with your doctor or ask to be referred to a therapist who specialises in sensory integration therapy. Weighted blanket material Weighted blankets are filled with two types of material: plastic pellets or glass beads.  Weighted blanket material
Weighted blankets are filled with two types of material: plastic pellets or glass beads. Glass beads are smaller – but heavier than plastic pallets. That small size has an advantage in that the blanket appears thinner. In contrast, plastic pellets are bigger, making the blanket a bit bulkier. However, blankets with plastic pallets are considerably cheaper since plastic is inexpensive compared to glass. Some weighted blankets come with other materials, such as polyester fibrefill or fleece lining, for an extra layer of warmth. If you’re planning to use the blanket during the cold winter months, this might be a nice perk. Removable cover Due to the weight of the blankets, they are bulky and hard to wash, which means a removeable cover is ideal. Cotton covers make for cool, breathable blankets, while other fabrics may best suit that warm and cosy feel. Sometimes, sellers will price covers as an add-on, so never assume your blanket comes with a removable cover. Adapted from an article by Esteban Vaquera. Medically reviewed by Brittany Stopa, MPH. Available at: www.symptomfind.com How good design can make aged care facilities feel more like home The stark difference between an aged care ‘home’ and a real home has been laid bare by the Covid pandemic from Aged Care New Zealand Issue 2 2022  Residential aged care buildings are often institutionally designed even if they have the appearance of a hotel. Think long corridors, vast dining rooms, nursing stations and bland corporate furnishings. These design choices support a model of care underpinned by cost efficiencies rather than real people’s rhythms of daily life. So, how can we make aged care facilities feel more like home, while keeping them pandemic safe? More like a ‘container’ than a home Residential aged care facilities are deeply restrictive environments. Some have compared them to prisons. During the pandemic, things were made worse as residents were denied the right to leave their rooms or have visitors. For many residents, it must feel like prevention is worse than the disease, as physical and psychological health declines markedly in imposed isolation. Hotel like residential aged care rooms are no place for long periods without the company of others. Some residential aged care centres may look like luxury resorts, but residents are still incarcerated. Often residential aged care centres are more like a ‘container’ than a home; a container that dispenses shelter, food and medical care. So what might we do differently in the post-pandemic era? To try to answer this question, we held a collaborative design workshop involving architects and stakeholders, including managers from the residential aged care sector. We sought to visualise design ideas using three existing not for profit residential aged care sites as testing grounds. We asked the group to ponder: what makes a home ‘home like’? And how does that differ from the environment at an aged care centre? Three key ideas emerged, all of which could help a facility feel more like a ‘container’ than a home while also reducing the impact of future pandemics.
Residential aged care facilities are often walled and gated enclaves set apart from the surrounding community. Residents are secluded in wards and aren’t part of the natural ebb and flow of the community. A home, on the other hand, is usually directly connected to the outside world. Embedding indistinguishable residential care households in the heart of an active community would add to the broader social and physical fabric and build support networks. In practice, this could mean opting for smaller buildings that look similar to surrounding buildings, rather than large and imposing structures. It could mean offering a wide range of housing choices from houses to apartments, and softening wall and gate barriers so residents easily connect with everyday community life.
Our group took inspiration from the urban design concept known as the ‘five-minute community’ where everything is a short walk away. We imagined designs that allow for self-sufficient small households of up to eight residents, with different generations also located in the same street. ‘Ageless’ communities like this allow for different generations to interact (either incidentally or deliberately). Residents could easily adjust the level of support needed (up and down) over time, while staying at home. Intensive rehabilitation could be delivered in the home or nearby. For example, people who have had a fall could access rehabilitation and restorative services in the local area. We also looked for ways to take advantage of existing spaces in the community rather than constructing new aged care facilities that are set apart.
Big isn’t always better. Small home models deliver an antidote to isolation and the spread of airborne respiratory infection. Smaller stand-alone buildings are less reliant on centralised air-circulation systems and can deliver strategies to reduce infection transmission by ensuring all rooms have access to fresh air and natural ventilation. Smaller households can quarantine without the need to lock down a large facility. Community participation and engagement built into the design Entrenched approaches to residential aged care design assumes residents can do little independently. An unquestioning focus on inabilities further disempowers: ‘care’ is done ‘to’ or ‘for’ a resident in a ‘facility’.  For example, residential aged care meals are generally pre-prepared and eaten in a large-scale room with many others (including strangers).
At home, by contrast, people decide what, when and where to eat. The small home approach in five-minute communities would allow, for instance, people of different generations to cook together or for a younger person to cook for an older person while learning new skills. Designs that acknowledge older people have knowledge and skills to contribute allow for such interactions to occur. When workshop participants challenged their own expectations, they envisioned design concepts emphasising living, not just existing, until end of life. The residential aged care crisis is escalating, and structural and cultural change is desperately needed. It’s time to rethink these physical environments with peoples’ fundamental human needs at the heart of design. Authors; Rosemary Kennedy Adjunct Professor of Architecture and Urban Design, Queensland University of Technology. Laura Buys, Honorary Professor, The University of Queensland This article is republished from The Conversation under a Creative Commons license. Read the original article here: theconversation.com//how-good-design-can-make-aged-care-facilities-feel-more like-home-176-465 |
AuthorShonagh O'Hagan Archives
July 2024
|
 RSS Feed
RSS Feed